Beyond Statistics, Towards Solutions
Why Maternal and Child Health Remains Maharashtra’s Toughest Tribal Challenge
Maharashtra has dramatically reduced maternal and child mortality over the last two decades. Yet tribal communities continue to face disproportionate risks from geography, poverty, poor connectivity and healthcare access. Part II of TheNews21’s Tribal Maharashtra series examines why progress remains uneven.Mumbai :
For a pregnant woman living in Mumbai, childbirth usually begins with a phone call, a short journey to a hospital and the reassurance that trained medical professionals are only minutes away. For a pregnant woman living in a remote tribal hamlet of Nandurbar, Palghar, Melghat or Gadchiroli, the experience can be very different. A swollen river may separate her village from the nearest road. A forest track may become impassable during the monsoon. A health centre that appears nearby on an official map may require hours of travel across difficult terrain. In such circumstances, access to healthcare is not simply a matter of availability. It becomes a matter of geography, connectivity and time.
This reality lies at the heart of Maharashtra’s tribal health challenge.
The Maharashtra State Tribal Health Committee Report presents a picture that is both encouraging and troubling. On one hand, the state has achieved remarkable progress in maternal and child health over the past two decades. Maternal mortality has fallen sharply. Infant mortality has declined. Institutional deliveries have become more common. Antenatal care has expanded. On the other hand, tribal communities continue to bear a disproportionate burden of risk, particularly during pregnancy, childbirth and early childhood.
The story of maternal and child health in tribal Maharashtra is therefore not a story of failure. Nor is it a story of complete success. It is a story of progress that remains unfinished.
One of the most important findings of the committee report is that Maharashtra’s public-health system has delivered measurable improvements in child survival. The under-five mortality rate among Scheduled Tribes has fallen dramatically over the last two decades. According to the report, under-five mortality among Scheduled Tribe children declined from 92.3 deaths per 1,000 live births during the NFHS-2 period to 37.3 during NFHS-5. The reduction is substantial and reflects years of investment in immunisation, maternal healthcare, nutrition interventions and frontline health services.
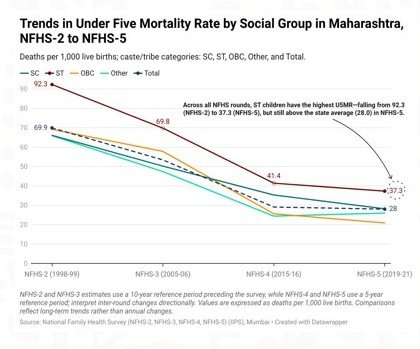
Yet the report also highlights an uncomfortable reality. Despite this progress, Scheduled Tribes continue to record the highest under-five mortality among all major social groups in Maharashtra. The numbers tell a story of improvement. They also tell a story of continuing inequality.
Public-health experts often describe the first five years of life as the most important period in human development. It is during these years that nutrition, disease prevention, vaccination coverage and access to healthcare shape not only survival but lifelong physical and cognitive development. For tribal children, however, several vulnerabilities often converge simultaneously. Many are born into households facing poverty. Many live in remote settlements. Some face barriers in accessing healthcare during critical stages of pregnancy and infancy. Others encounter nutritional deficits that begin before birth and continue through childhood. The result is that geography and circumstance continue to influence health outcomes far more than they should in a modern healthcare system.
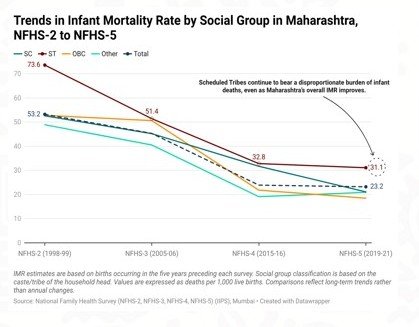
The committee report reveals a similar pattern in infant mortality. Infant mortality among Scheduled Tribes has declined dramatically over the past two decades, falling from 73.6 deaths per 1,000 live births during NFHS-2 to 31.1 during NFHS-5. This represents one of the most significant public-health achievements recorded in the report. Yet even after this decline, tribal communities continue to experience infant mortality levels above those observed among many other social groups. For policymakers, this presents a difficult challenge. The question is no longer whether interventions work. The evidence clearly demonstrates that they do. The challenge is understanding why tribal communities continue to lag despite decades of improvement. Part of the answer lies in geography.
The committee’s field visits repeatedly encountered settlements located across difficult terrain where rivers, hills and forests create barriers between communities and healthcare services. Photographs included in the report show health workers travelling long distances to provide immunisation and patients being transported across difficult landscapes using bamboo stretchers. These images are not merely illustrations. They represent the daily realities of healthcare delivery in some of Maharashtra’s most remote regions.
Retired IAS officer Pradeep Vyas, who worked extensively in both the health and tribal development sectors, argues that the challenge is not simply one of resources. Many tribal settlements are dispersed across hills and forests, making access difficult despite relatively short physical distances. A location that appears only a few hundred metres away in a straight line may require hours of travel because of terrain and settlement patterns. This distinction is important.
A Primary Health Centre (PHC) may exist within prescribed service norms. A family may still struggle to reach it when needed. The consequences become particularly serious during pregnancy and childbirth.
Few public-health interventions have contributed more to reducing maternal and neonatal deaths than institutional deliveries. Deliveries conducted in healthcare facilities increase the likelihood that complications will be identified and treated promptly. Access to skilled birth attendants, emergency referral systems and basic obstetric care dramatically improves outcomes for both mothers and newborns.
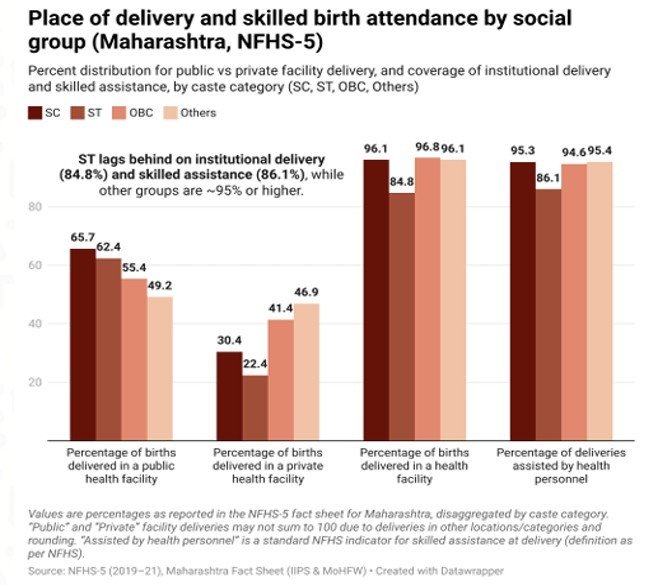
The committee report shows that institutional delivery coverage among tribal communities has improved substantially. However, Scheduled Tribes continue to lag behind several other social groups. While more than 95 percent of births among many social groups now occur in health facilities, institutional delivery among Scheduled Tribes remains lower at 84.8 percent. The gap may appear modest on paper. In practice, it represents thousands of births occurring outside the healthcare system.
Former Public Health Minister Dr Deepak Sawant, who has spent decades working in tribal regions, believes accessibility remains one of the most important barriers to institutional deliveries. According to Dr Sawant, transportation challenges continue to affect timely access to healthcare facilities in several remote areas. During his tenure, efforts were made to introduce motorcycle ambulance services in difficult terrain where conventional ambulances could not easily operate. His observation highlights a recurring theme throughout the committee report.
The challenge facing tribal healthcare is often not the absence of facilities. It is the difficulty of reaching them. The importance of accessibility becomes even more evident when one examines maternal healthcare indicators.
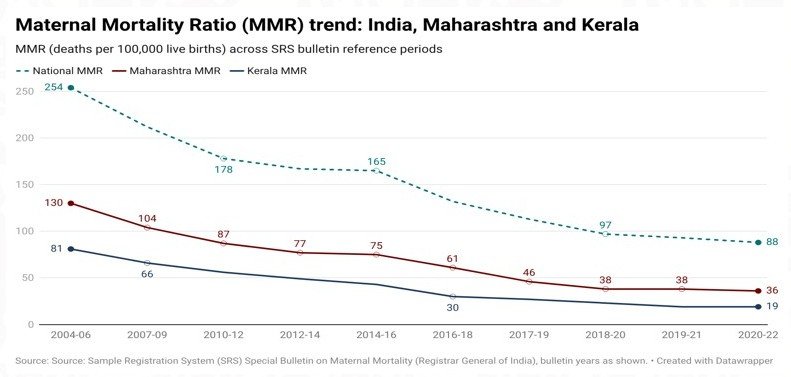
One of Maharashtra’s most significant public-health achievements has been the steady reduction in maternal mortality. The committee report shows that the state’s Maternal Mortality Ratio (MMR) declined from 130 deaths per 100,000 live births during 2004-06 to 36 during 2020-22. During the same period, India’s national MMR fell from 254 to 88. These figures reflect decades of investment in maternal healthcare, institutional deliveries, skilled birth attendance and emergency obstetric care. Measured purely through statistics, Maharashtra’s progress appears impressive. Yet averages often conceal inequalities.
The committee report’s district-level analysis demonstrates that maternal health outcomes vary considerably across the state. Some districts continue to experience significantly higher risks than others, reminding policymakers that statewide success does not necessarily translate into uniform progress on the ground. For tribal women, pregnancy remains intertwined with challenges that extend far beyond healthcare facilities. Distance, transportation, nutrition, poverty and access to timely medical intervention continue to shape outcomes. The committee’s analysis of antenatal care indicators provides further insight into these realities. Antenatal care is often described as the foundation of maternal health. It is during pregnancy that healthcare workers identify high-risk cases, monitor nutritional status, detect anaemia and intervene before complications become life-threatening.
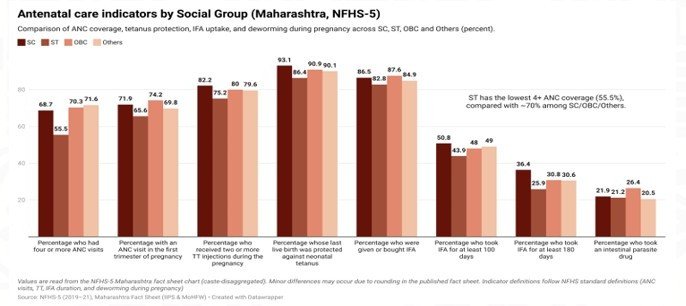
The report shows encouraging progress in several areas. A majority of tribal women now receive antenatal care, undergo health check-ups and access institutional healthcare during pregnancy. Yet the data also reveal persistent gaps when compared with other social groups. Scheduled Tribe women continue to record lower coverage in several antenatal care indicators. The report specifically highlights lower antenatal care coverage among tribal communities compared with Scheduled Castes, OBCs and other groups. These gaps matter because maternal health problems rarely emerge suddenly. They develop gradually.
A woman suffering from severe anaemia does not become anaemic overnight. A high-risk pregnancy often presents warning signs weeks or months before delivery. Timely identification and intervention can prevent complications that might otherwise become fatal. This is why former Public Health Minister Dr Deepak Sawant believes haemoglobin monitoring deserves far greater attention within tribal healthcare programmes. Drawing upon decades of experience in public health and tribal regions, Dr Sawant argues that regular haemoglobin estimation among students in Ashram schools and pregnant women should become a priority. He particularly emphasises monitoring during the final trimester of pregnancy, when maternal health directly influences birth outcomes. His concern reflects one of the report’s recurring themes.
The battle for child survival often begins before a child is born. Maternal anaemia increases the risk of premature delivery, low birth-weight babies and complications during childbirth. It weakens both mother and child, creating vulnerabilities that can persist long after delivery. The consequences extend beyond mortality statistics. They affect cognitive development, educational outcomes, physical growth and future productivity.
In many respects, maternal health is the foundation upon which child health is built. Yet healthcare interventions alone cannot fully address these challenges. The committee’s field observations repeatedly demonstrate that geography continues to influence outcomes in ways that conventional policy frameworks often underestimate.
For much of urban Maharashtra, the monsoon is an inconvenience. For many tribal communities, it can become a public-health emergency. During heavy rains, rivers swell beyond safe crossing levels. Mud roads become impassable. Transportation slows dramatically. Entire settlements can become temporarily isolated from nearby healthcare facilities.
The committee’s photographs of bamboo-lance patient transport systems are striking precisely because they illustrate realities that rarely appear in policy documents. They reveal the extraordinary lengths to which families and healthcare workers sometimes go to secure medical assistance.
A woman entering labour cannot postpone childbirth until weather conditions improve. A child suffering from severe illness cannot wait for floodwaters to recede. Healthcare access during these moments becomes a race against geography itself.
Dr Deepak Sawant recalls that accessibility challenges in tribal regions led to the introduction of motorcycle ambulance services in difficult terrain during his tenure. Such innovations recognised an important truth: conventional solutions do not always work in unconventional landscapes.
The challenge facing tribal healthcare is therefore not merely the construction of more facilities. It is ensuring that those facilities remain accessible when communities need them most. The committee’s findings also highlight another dimension that is frequently overlooked in discussions about health outcomes.
Poverty.
Health planners often focus on hospitals, medicines and healthcare personnel. Families, however, frequently make decisions based on economics. Dr Sawant points to the example of Nutrition Rehabilitation Centres established for severely malnourished children. Despite the importance of these facilities, utilisation often remains lower than expected in some areas.
One reason is simple. For a daily-wage household, accompanying a child to a rehabilitation centre may mean losing income. A mother staying with a child cannot work. A father may be reluctant to leave employment for extended periods. Travel expenses create additional burdens. The consequence is a tragic paradox. The families most in need of nutritional interventions are often the least able to bear the economic costs associated with accessing them.The same logic applies to antenatal visits, institutional deliveries and follow-up care.
Every interaction with the healthcare system carries an opportunity cost for households already living under economic pressure. This reality reminds us that health policy cannot be separated from livelihoods. A malnourished child is rarely the result of a single failure. It is often the outcome of interconnected challenges involving nutrition, income, transportation, education and healthcare access.
The committee report also draws attention to an issue that policymakers often struggle to address: trust.
Across many tribal regions, traditional healers, local practitioners and culturally embedded systems of care continue to play important roles within communities. These systems are not merely healthcare mechanisms. They are part of social and cultural life. Dr Sawant notes that traditional healers continue to influence healthcare-seeking behaviour in several tribal regions. Their presence reflects longstanding relationships of trust developed over generations.
The policy challenge, therefore, is not confrontation. It is engagement.
Successful public-health programmes are rarely those that dismiss existing belief systems. They are the ones that gradually build confidence in modern healthcare while respecting local realities and community structures.
The committee’s emphasis on community engagement reflects this understanding. Healthcare systems function most effectively when communities view them as trusted partners rather than distant institutions. The broader lesson emerging from the report is that tribal health cannot be understood solely through hospitals and healthcare facilities.
Health outcomes are shaped by roads, transportation, nutrition, education, communication networks, livelihoods and social trust. A functioning bridge may save as many lives as a health centre. A mobile communication tower may improve emergency response as effectively as additional equipment. A nutrition intervention may prevent illnesses that no hospital can fully cure.
The Maharashtra State Tribal Health Committee Report therefore presents a challenge not only to the Health Department but to the entire governance system.
Its findings suggest that improving tribal health requires coordinated action across multiple sectors rather than isolated interventions within healthcare alone. At the same time, the report offers reasons for optimism.
The dramatic decline in maternal mortality, infant mortality and under-five mortality demonstrates that progress is possible. Thousands of children are alive today because healthcare systems improved. Thousands of mothers survive pregnancy because interventions that were unavailable a generation ago now exist.
These achievements deserve recognition. But they should not create complacency. The journey towards health equity remains unfinished. The challenge before Maharashtra is no longer proving that improvement is possible. The challenge is ensuring that every mother and every child, regardless of how remote their settlement may be, benefits from that progress.
Because in a state that aspires to become a model of development, no child’s future should be determined by how far they are born from the nearest road.
Next Part
Part III: The Anaemia Generation — Why Malnutrition Continues to Haunt Tribal Maharashtra

{kind=link}