Beyond the Toilet
Why Sanitation Remains an Unfinished Story in Tribal Maharashtra
A toilet is more than a household facility. It is linked to health, dignity and disease prevention. Part V of the Tribal Maharashtra series explores why sanitation remains an unfinished story in many tribal regions despite years of progress.
For most people, a toilet is a simple household facility. It is so commonplace that its presence is rarely noticed. Its absence, however, changes everything. It affects the health. It affects the dignity. It affects safety and in many cases, it affects the future of a child.
Over the past decade, Maharashtra has witnessed a significant expansion in sanitation infrastructure. Thousands of villages have been declared open-defecation free, millions of toilets have been constructed and access to sanitation has improved across much of the state. On paper, the sanitation story appears to be one of remarkable progress. But the Maharashtra State Tribal Health Committee Report reveals a more complex reality.
The challenge in tribal Maharashtra is no longer merely about constructing toilets. Increasingly, it is about ensuring that they can actually be used. The report’s findings on Water, Sanitation and Hygiene (WASH) highlight an important but often overlooked dimension of tribal health. Historically, sanitation practices in tribal areas have been shaped by settlement patterns, ecological conditions and local customs. In many remote regions, dispersed settlements and the absence of household latrines contributed to a long-standing dependence on open defecation.
Government programmes have substantially expanded toilet coverage over the years. Yet access and usage have not progressed uniformly. The gap becomes visible when sanitation indicators are examined across different social groups.
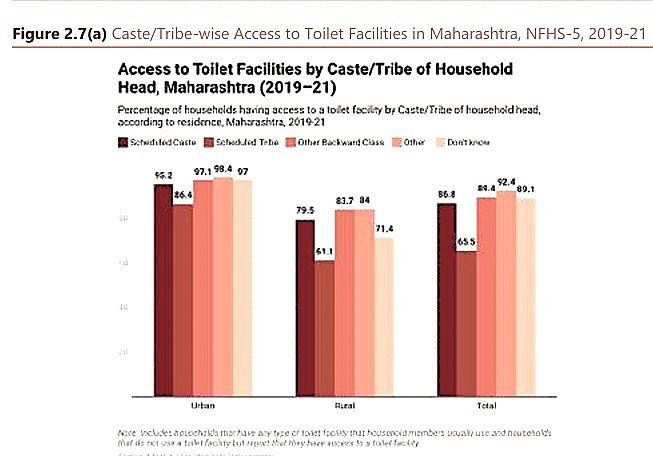
According to NFHS-5 data cited in the report, Scheduled Tribe households continue to record the lowest levels of toilet access among all major social groups in Maharashtra. The disparity is particularly striking in rural areas. While 79.5 per cent of rural Scheduled Caste households report access to a toilet facility and the figure rises to 83.7 per cent among OBC households and 84 per cent among other social groups, only 61.1 per cent of rural Scheduled Tribe households report similar access.
The difference is substantial. It means that nearly four out of every ten rural tribal households continue to remain outside the sanitation coverage enjoyed by large sections of rural Maharashtra. Even when urban and rural households are combined, the gap remains visible. Overall toilet access among Scheduled Tribe households stands at 65.5 per cent, compared with 86.8 per cent among Scheduled Castes, 89.4 per cent among OBCs and more than 92 per cent among households classified under the ‘Other’ category.
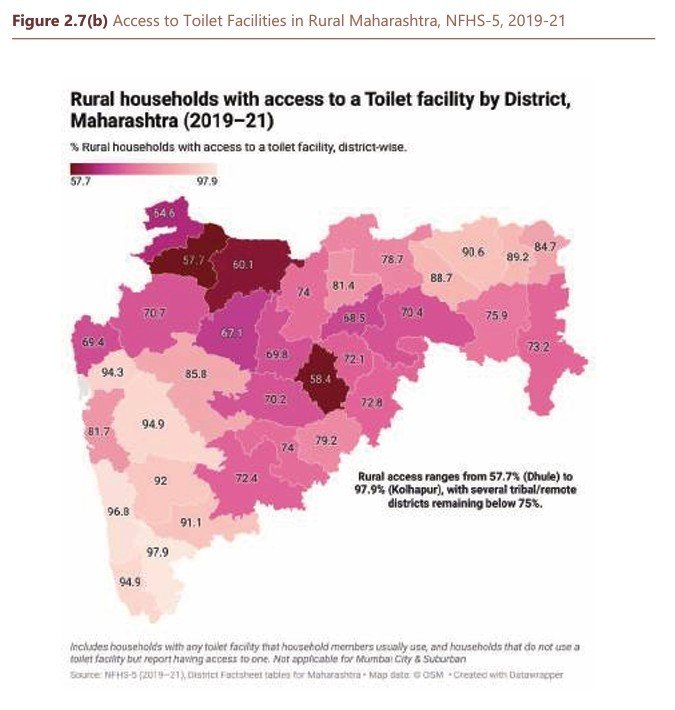
These are not merely sanitation statistics. They are indicators of deeper inequalities in access to basic household amenities. The report suggests that sanitation gaps in tribal communities are often linked to broader infrastructural disadvantages that directly influence health outcomes, disease prevention and quality of life. The district-level picture tells a similar story.
The report’s mapping of rural toilet access across Maharashtra reveals sharp geographical variations. While some districts approach near-universal access, several interior and relatively remote districts continue to record substantially lower levels of coverage. The pattern is not random. Many of the districts with lower sanitation access overlap with regions that have historically faced challenges related to terrain, remoteness and service delivery.
The findings reinforce a theme that has repeatedly emerged throughout this series. Whether the issue is maternal health, child nutrition, anaemia or access to healthcare, tribal communities often experience development differently from the state average. The challenge is rarely the complete absence of progress. The challenge is that progress does not always reach every household at the same pace. That distinction is important. Because the story emerging from the Committee’s report is not one of failure.
It is a story of uneven development and nowhere is that unevenness more visible than in the seemingly simple question of whether a household has access to a toilet. Yet the report also warns against drawing quick conclusions. The next challenge is even more complicated. Because in tribal Maharashtra, building a toilet is often easier than ensuring that it can be used consistently and that is where the sanitation story becomes a public health story.
The report’s most important insight, however, lies beyond the numbers. Because sanitation in tribal Maharashtra is not simply a question of whether a toilet has been constructed. It is a question of whether that toilet can actually be used. This distinction is crucial.
Across India, sanitation programmes have often been measured through the number of toilets built. Construction figures are easy to record, targets are easy to monitor and progress can be quantified. Usage is far more complicated. The Tribal Health Committee Report repeatedly suggests that sanitation outcomes in tribal areas are shaped not merely by infrastructure creation but by the conditions that surround that infrastructure. Water availability is one such factor.
In many tribal regions, particularly those located in hilly and forested terrain, seasonal water scarcity continues to affect everyday life. When water itself becomes a scarce resource, household priorities inevitably shift. Drinking water comes first. Cooking comes next. Water for livestock often follows. In such circumstances, the regular use and maintenance of household toilets may become more difficult.
The report specifically notes that seasonal water shortages can constrain toilet usage, particularly in remote settlements where access to reliable water supply remains limited. The challenge does not end there. Several state and district reviews conducted under the Swachh Bharat Mission Phase II have highlighted another problem. A significant proportion of toilets in remote tribal gram panchayats either require maintenance or need retrofitting because of unsuitable terrain, soil conditions and the absence of reliable pit-emptying services.
In other words, a toilet may exist on paper and even physically within a household, but that does not necessarily mean it remains functional over time. This is particularly relevant in tribal regions where geography continues to shape development outcomes. The same hills, forests and scattered settlements that make healthcare access difficult also affect sanitation infrastructure. A design that works in a densely populated urban settlement may not necessarily function effectively in a remote tribal hamlet.
The report points to another often overlooked issue. Electricity and lighting. For many urban households, these may appear unrelated to sanitation. Yet in several remote regions, inadequate lighting can influence whether toilets are comfortably used during early mornings or after sunset, particularly by women and elderly residents. The result is a situation where infrastructure may be available, but utilisation remains inconsistent.
This finding challenges one of the most common assumptions in public policy. The assumption that infrastructure automatically translates into outcomes. The report suggests that reality is more complex. A toilet without water is difficult to use. A toilet without maintenance eventually becomes unusable. A toilet constructed without considering terrain may require repeated repairs and a toilet that does not fit local conditions may gradually fall out of use. This is why the report argues that sanitation outcomes in tribal regions are shaped less by cultural resistance than by the absence of enabling conditions.
For years, discussions around sanitation in rural India often focused on behavioural change. The Committee’s findings offer a broader perspective. They suggest that when assured water supply, appropriate toilet design and maintenance systems are available, usage becomes significantly easier to sustain. Where these supporting conditions are absent, even well-intentioned sanitation programmes struggle to achieve their full public health impact. The implications extend far beyond sanitation itself. Because the moment a toilet becomes difficult to use, the issue moves from infrastructure to health and that is where the story begins to connect with everything that this series has explored so far — maternal health, child survival, malnutrition and quality of life.
What appears to be a sanitation challenge is, in reality, part of a much larger public health equation and this is where sanitation ceases to be merely an infrastructure issue. It becomes a health issue. A dignity issue and ultimately, a development issue.
Throughout this series, the Maharashtra State Tribal Health Committee Report has repeatedly highlighted how different challenges in tribal regions are interconnected. Maternal health cannot be separated from nutrition. Nutrition cannot be separated from disease. Disease cannot be separated from access to healthcare and sanitation cannot be separated from any of them.
The links are often invisible until something goes wrong. A child suffering from malnutrition becomes more vulnerable to infections. A pregnant woman faces greater health risks when sanitation facilities are inadequate. A family without access to safe sanitation remains more exposed to conditions that can undermine months of nutritional and healthcare interventions.

Public health experts have long argued that disease prevention begins long before a patient reaches a hospital. The Committee’s findings reinforce that view. Sanitation is not simply about convenience. It is one of the first lines of defence against illness. That is why the report repeatedly connects sanitation outcomes with broader questions of health, dignity and disease prevention. The issue becomes particularly significant for women.
In many remote settlements, the absence of reliable and consistently usable sanitation facilities affects privacy, safety and everyday well-being. The report notes that inadequate lighting, water shortages and difficult terrain can all influence usage patterns, particularly during early mornings and after sunset. What appears to be a household amenity therefore becomes a question of personal dignity. The challenge also extends to children.
Throughout Parts II and III of this series, we examined maternal health, child mortality, anaemia and malnutrition. The sanitation chapter reveals how many of those issues are linked through pathways that are often overlooked.
Former Public Health Minister Dr. Deepak Sawant recently drew attention to one such connection while reflecting on conditions in parts of Melghat. According to him, water scarcity continues to affect several remote regions, forcing families to travel long distances in search of water. Such conditions can increase vulnerability to water-borne diseases. For a child already suffering from Severe Acute Malnutrition (SAM) or Moderate Acute Malnutrition (MAM), even a single episode of diarrhoea can significantly worsen health outcomes.
His observation adds an important practical dimension to the Committee’s findings. It reminds us that public health challenges rarely exist in isolation. A shortage of water can become a sanitation problem. A sanitation problem can become a disease burden. Disease can aggravate malnutrition and malnutrition can ultimately affect survival itself.
The chain is continuous. So are the consequences. The sanitation chapter of the report therefore offers a broader lesson. Development cannot be measured only by the number of facilities created. The more important question is whether those facilities function in the realities of everyday life. Can water be accessed consistently? Can the toilet be maintained? Can it be used safely? Can it continue serving the household year after year?
These questions may appear simple. Yet they often determine whether public investments translate into lasting improvements in health. The story of sanitation in tribal Maharashtra is therefore not a story of absence. It is a story of unfinished progress. Toilets have been built. Coverage has improved. The gap has narrowed. But the Committee’s findings make it clear that the journey is not complete.
As Maharashtra continues to improve healthcare, nutrition and service delivery in tribal regions, sanitation will remain a critical part of that effort. Because public health does not begin in a hospital ward. It begins at home. It begins with clean surroundings. It begins with safe sanitation and sometimes, the distance between health and illness is measured not by kilometres travelled or medicines prescribed, but by something as simple as a functioning toilet.
That may be one of the most important lessons emerging from the Tribal Health Committee Report and one of the most important reminders for policymakers seeking to build a healthier future for tribal Maharashtra.

{kind=link}