The Anaemia Generation: Why Malnutrition Continues to Shadow Tribal Childhood
The battle against malnutrition often begins before birth. Part III of TheNews21’s Tribal Maharashtra series explores anaemia, stunting, wasting and the deeper structural challenges that continue to affect tribal children across Maharashtra
Mumbai: Long before a child learns to walk, speak or attend school, another story is already being written. It is written quietly, often invisibly. In the blood of a pregnant mother. In the food available at home. In the distance between a remote hamlet and the nearest health centre and sometimes, in the difficult choices that families make between earning a day’s wage and seeking medical care.
By the time a child is identified as malnourished, the problem may already be years old. That is perhaps the most important lesson emerging from the Maharashtra State Tribal Health Committee Report.
The report shows that Maharashtra has made significant progress in reducing child malnutrition over the last two decades. Yet it also reveals a troubling reality: thousands of tribal children continue to begin life at a disadvantage. The challenge is no longer simply one of food scarcity. It is increasingly a question of nutrition, maternal health, anaemia, healthcare access and the ability of public services to consistently reach the most remote communities. Nowhere is this reality more visible than in the data on anaemia.
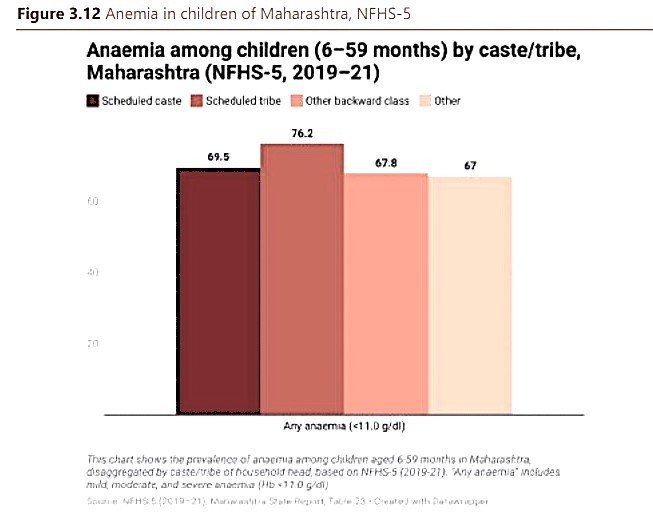
According to the report, 76.2 per cent of Scheduled Tribe children between six and fifty-nine months of age are anaemic. The figure is startling. It means that roughly three out of every four tribal children in Maharashtra suffer from a condition that weakens immunity, affects physical growth and reduces cognitive development. Unlike many childhood illnesses, anaemia rarely announces itself dramatically. It grows quietly. A child may appear tired. Concentration may suffer. Learning ability may decline. Physical growth may slow. Yet the cumulative impact can shape an entire childhood.
For Dr. Deepak Sawant, former Maharashtra Health Minister and current Chairman of the Task Force on Malnutrition Eradication, this is where the battle against malnutrition must begin. In his view, regular haemoglobin testing among Ashram School students and systematic monitoring of pregnant women should become one of the state’s highest priorities. His concern reflects a reality that public health experts have long understood.
Malnutrition often begins before birth. A pregnant woman suffering from anaemia is more likely to face complications during pregnancy. The risk of low birth weight increases. The child may enter the world already vulnerable, carrying disadvantages that nutrition programmes later struggle to overcome. In other words, the story of an undernourished child frequently begins with the health of the mother. The report repeatedly points towards this connection.
While healthcare services have expanded considerably over the years, the burden of nutritional deprivation continues to fall disproportionately on tribal communities. The challenge becomes particularly acute in remote settlements where geography itself acts as a barrier.
A pregnant woman living in a city can access diagnostic services, specialist consultations and emergency care relatively quickly. For a woman living in a scattered tribal hamlet in Nandurbar, Palghar, Melghat or Gadchiroli, the journey can be very different. Distance is measured not merely in kilometres, but in travel time. Road conditions matter. Seasonal rivers matter. Transport availability matters and often, so does the family’s economic situation.
The committee’s findings suggest that healthcare access and nutrition cannot be viewed separately. They are deeply interconnected. A woman who misses antenatal check-ups is less likely to have anaemia detected early. A child born with low birth weight is more vulnerable to growth deficits. A family struggling with poverty may delay seeking care until the condition becomes severe. Each challenge reinforces the next.
This is why Dr. Sawant argues that tribal health policy must move beyond simply counting the number of nutrition schemes or healthcare centres. The real question is whether those interventions are reaching vulnerable families early enough. By the time severe malnutrition becomes visible, opportunities for prevention may already have been lost.
The report’s findings on child nutrition underline the scale of the challenge. While Maharashtra has undoubtedly improved health outcomes over time, tribal children continue to experience significantly higher levels of nutritional stress than many other groups. The state’s success story is therefore incomplete. The numbers show progress. But they also reveal a generation still growing up under the shadow of anaemia and nutritional deprivation and it is that generation whose future now forms one of the most important development challenges facing Maharashtra.
A Childhood Shaped by Malnutrition
For most parents, a child’s growth is measured through small milestones. The first steps. The first words. The first day of school. A little more height every year. A little more strength. A little more confidence. Yet for thousands of tribal families, another reality often unfolds alongside these milestones.
A child may survive infancy. A child may avoid serious illness. A child may even attend school regularly. But growth itself may remain compromised. This is where malnutrition becomes particularly difficult to understand.
Unlike a fever or an infection, it does not always appear as an immediate crisis. Its effects accumulate gradually. Month after month. Year after year and by the time the consequences become visible, much of the damage has already been done.
The Maharashtra State Tribal Health Committee Report captures this reality through one of the most important indicators in child nutrition: stunting. In simple terms, stunting reflects chronic undernutrition. It indicates that a child has not received adequate nutrition over a prolonged period and, as a result, has failed to achieve expected physical growth.
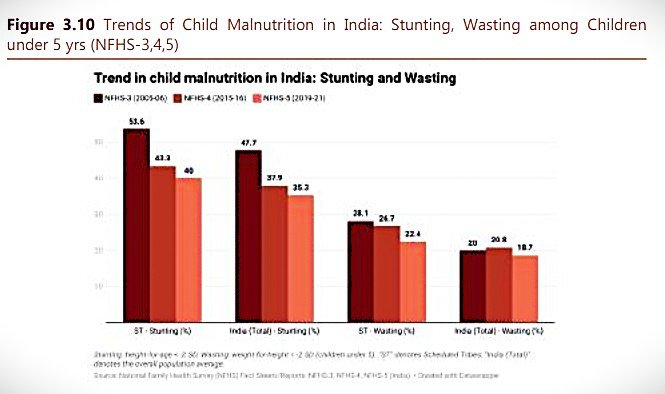
The report shows that tribal Maharashtra has made undeniable progress. Among Scheduled Tribe children, stunting declined from 53.6 per cent during NFHS-3 to 42.3 percent during NFHS-4 and further to 40 per cent during NFHS-5. The trend is encouraging. It reflects years of investment in maternal healthcare, immunisation, nutrition programmes, Anganwadi services and community outreach.
Thousands of children are undoubtedly healthier today than they would have been two decades ago. Yet the numbers also reveal a harsher truth. Even after years of improvement, four out of every ten tribal children remain stunted. For policymakers, this should be a sobering statistic. A stunted child is not merely shorter than average. Research across the world has consistently shown that chronic undernutrition affects cognitive development, educational performance, physical capacity and long-term productivity. The consequences extend far beyond childhood. They can influence an individual’s entire life trajectory.
The report’s findings on wasting present an equally troubling picture. Unlike stunting, which develops gradually over time, wasting reflects acute nutritional stress. It often indicates that a child is not receiving enough food or is repeatedly affected by illness. Among tribal children, wasting declined from 28.1 per cent during NFHS-3 to 22.4 per cent during NFHS-5. Again, the direction is positive. But the level remains alarmingly high. Nearly one in every four tribal children continues to face acute nutritional vulnerability and for those children, the risks are immediate.
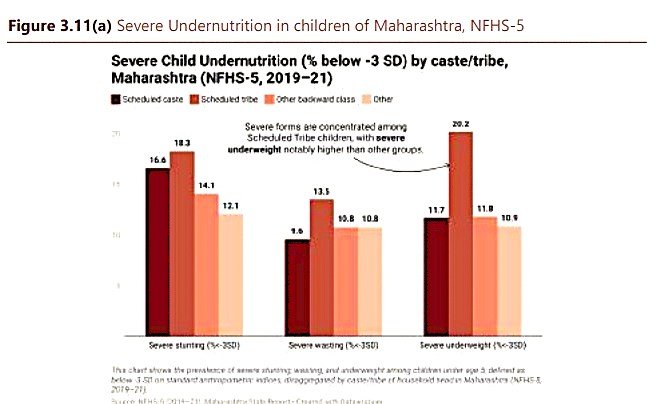
Severe wasting is associated with increased susceptibility to infections, weakened immunity and higher mortality risks. In many ways, wasting is the nutritional equivalent of a warning signal. It indicates that a child’s health is under active stress. The committee’s data becomes even more concerning when it examines severe forms of undernutrition. Among Scheduled Tribe children under five years of age, severe stunting affects 18.3 per cent. Severe wasting affects 13.5 per cent. Most strikingly, severe underweight prevalence stands at 20.2 per cent. These are not marginal numbers. They represent children facing the highest levels of nutritional deprivation.
In practical terms, one out of every five tribal children falls into the category of severe underweight. That reality should concern not only public-health officials but every department connected with tribal development, education, food security and social welfare. Because severe undernutrition is not simply a health indicator. It is often the visible outcome of multiple systems failing simultaneously. A child may be born with low birth weight. The family may struggle with poverty. Nutrition services may not reach consistently. Healthcare access may be limited. Education levels may be low. Safe drinking water may be unavailable.
When these factors converge, undernutrition becomes almost inevitable. This is why experts increasingly argue that malnutrition cannot be solved through nutrition schemes alone. The challenge is larger than food distribution. It involves livelihoods. It involves sanitation. It involves maternal health and it involves governance.
Dr. Deepak Sawant’s observations fit squarely within this broader understanding. His emphasis on haemoglobin monitoring is significant because it shifts attention upstream. Rather than waiting for severe malnutrition to emerge, he argues for identifying risk factors early. The logic is simple. A child who begins life with adequate birth weight, better maternal nutrition and stronger early healthcare support has a far greater chance of avoiding the cycle of malnutrition altogether.
Prevention is not only more effective than treatment. It is also far less expensive. Yet prevention remains difficult in regions where healthcare workers must cover vast and scattered populations. The committee report repeatedly highlights this challenge. Reaching every child in a dense urban settlement is difficult. Reaching every child across dozens of remote hamlets separated by hills, forests and seasonal rivers is an entirely different task. The burden on frontline workers is immense and yet much of Maharashtra’s progress has been achieved precisely because those workers continue to operate under challenging circumstances.
The result is a paradox that runs throughout the report. Maharashtra has succeeded in reducing malnutrition. But it has not yet succeeded in eliminating the structural conditions that produce malnutrition. That distinction matters. Because future progress will depend less on launching new schemes and more on ensuring that existing interventions consistently reach the children who remain most vulnerable. And nowhere does that challenge become more visible than in the everyday realities of nutrition delivery, poverty and access that continue to shape life across tribal Maharashtra.
Why Schemes Alone Are Not Enough
If the Maharashtra State Tribal Health Committee Report teaches one lesson above all others, it is that malnutrition cannot be solved by food distribution alone. For decades, governments have launched nutrition programmes, supplementary feeding schemes, Take Home Ration initiatives and special interventions for mothers and children. Many of these programmes have delivered measurable benefits. The decline in stunting, wasting and severe undernutrition would not have been possible without them. Yet the report repeatedly points towards a difficult reality.
The existence of a scheme does not automatically guarantee its effectiveness. What matters is whether the benefits reach the child at the right time, in the right quantity and in a form that can actually be used. This is where geography, poverty and administration often collide.
Dr. Deepak Sawant has spent years working in tribal regions, first as a legislator deeply involved in tribal issues and later as Maharashtra’s Public Health Minister. His observations reveal how implementation challenges can undermine even well-intentioned programmes. Take the example of nutrition support. In many remote tribal hamlets, delivering nutritional supplements is itself a logistical challenge. Some settlements remain difficult to access throughout the year, while others become virtually isolated during the monsoon. To overcome these barriers, supplies are often transported in bulk and distributed for extended periods. The intention is understandable. The difficulty lies in what happens next.
According to Dr. Sawant, nutritional supplements stored for weeks or months in humid conditions frequently face quality challenges. During the monsoon, moisture becomes an additional problem. In remote settlements where storage facilities are limited, preserving nutritional value becomes difficult. The result is a paradox that policymakers across the world have struggled with.
Food may reach the village. Nutrition may not always reach the child. This distinction is important. The success of a nutrition programme cannot be measured solely by the quantity distributed. It must ultimately be measured by outcomes. Are children healthier? Are anaemia levels falling? Are fewer children entering severe malnutrition? These are the questions that matter.
The committee report suggests that Maharashtra still has work to do. The challenge becomes even more visible in the functioning of Nutrition Rehabilitation Centres, or NRCs. These centres were established to provide intensive care and nutritional support to severely malnourished children. In theory, they represent one of the most important safety nets within the public-health system. Yet utilisation often remains lower than expected.
Dr. Sawant believes the reasons are not difficult to understand. A severely malnourished child does not arrive at an NRC alone. A mother usually accompanies the child. Sometimes another family member must also travel. For a family dependent on daily wages, this creates an immediate economic dilemma. Every day spent at a rehabilitation centre may be a day without income. Travel costs add to the burden. Household responsibilities remain unattended. For families already struggling to survive, seeking treatment can become a financial decision as much as a medical one. This reality highlights an uncomfortable truth.
The families most vulnerable to malnutrition are often the least able to absorb the economic costs associated with treatment. As a result, interventions that appear adequate on paper may not achieve the desired impact on the ground. This is not a failure of intent. It is a reminder that public policy must account for how people actually live. The report repeatedly demonstrates that malnutrition is rarely caused by a single factor. It is the outcome of multiple vulnerabilities operating simultaneously. Poor maternal nutrition. Anaemia. Low birth weight. Inadequate dietary diversity. Seasonal unemployment. Difficult terrain. Limited access to healthcare. Educational disadvantages.
Each factor reinforces the others and together they create conditions in which malnutrition becomes difficult to escape. This is why experts increasingly describe malnutrition not merely as a health problem but as a development problem. The child who enters school undernourished is more likely to struggle academically. The adolescent suffering from chronic anaemia is more likely to experience reduced physical capacity. The adult who grew up malnourished may face lifelong disadvantages in productivity and income. The consequences travel across generations. A malnourished girl may grow into an anaemic mother. An anaemic mother may give birth to a low birth-weight child and the cycle begins again.
Breaking that cycle requires more than nutrition schemes. It requires a comprehensive approach that brings together healthcare, education, livelihoods, sanitation, women’s empowerment and tribal development. The committee report offers several reasons for optimism. The progress achieved over the past two decades is substantial. Stunting has declined. Wasting has declined. Health services have expanded. Awareness has improved. Thousands of children are healthier today than previous generations. These achievements deserve recognition. But progress should not be confused with completion.
The report’s most powerful message may be that the final stretch is often the hardest. Reaching the easiest populations first is relatively straightforward. Reaching the last child in the last hamlet is far more difficult. Yet that is precisely where Maharashtra’s next challenge lies. For decades, development has often been measured through budgets, schemes and infrastructure projects. Those indicators remain important. But the true measure of success is simpler.
Can a tribal mother complete her pregnancy without anaemia? Can a child grow without being stunted? Can a family access nutritional support without sacrificing its livelihood? Can the circumstances of birth cease to determine the opportunities of life? These are the questions that ultimately matter.
The Maharashtra State Tribal Health Committee Report does not claim that the state has failed. Nor does it suggest that the problem is insurmountable. Instead, it presents a more nuanced reality. Maharashtra has travelled a considerable distance. But the journey remains unfinished and perhaps the most important lesson from this report is that the battle against malnutrition is not simply about feeding children. It is about creating the conditions in which every child has the opportunity to grow, learn and thrive. Because the future of tribal Maharashtra will not be decided by the number of nutrition schemes announced. It will be decided by whether the next generation of tribal children grows up healthier than the last.
Next Part
Part IV: Beyond the Health Centre
Why Geography, Infrastructure and Governance Continue to Shape Tribal Lives
The next article examines how roads, communications, transportation and administrative delivery influence health outcomes across Tribal Maharashtra.

{kind=link}