The Distance Between Life and Care
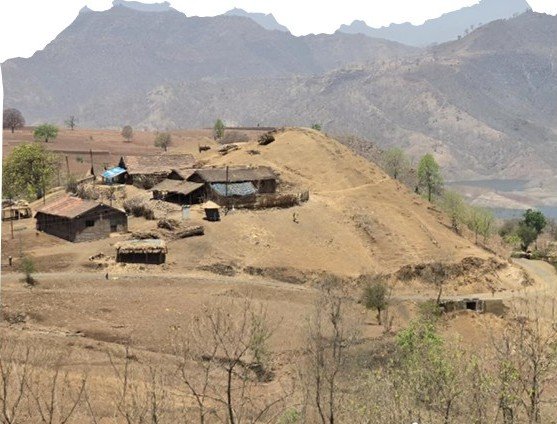
A child develops a high fever in Mumbai. Within minutes, parents can call a doctor, hail a taxi, visit a nearby clinic or reach a hospital emergency room. Hundreds of healthcare options exist within a few kilometres. Now imagine the same fever in a remote tribal hamlet perched on a hillside in Nandurbar, Palghar or Melghat. The illness is the same. The urgency is the same. The distance to care is not. For many tribal families, the first challenge is not finding a doctor. It is reaching one.
The Maharashtra State Tribal Health Committee Report repeatedly returns to a reality that rarely finds space in policy discussions. Tribal health is not merely about hospitals, medicines or doctors. It is also about geography. The map often decides outcomes long before medicine enters the picture. Scattered settlements, dense forests, seasonal rivers, mountainous terrain and isolated hamlets continue to shape everyday life across large parts of tribal Maharashtra.
The report’s field observations paint a picture far removed from the urban understanding of healthcare access. In many regions, villages are not concentrated settlements but clusters of small hamlets spread across hills, valleys and forests. A Primary Health Centre may officially serve a population, yet reaching that facility can involve hours of travel. The challenge is not unique to one district. It cuts across several tribal regions of Maharashtra.

Former IAS officer and State Information Commissioner for Greater Mumbai Dr Pradeep Vyas, who has worked extensively in both tribal development and public health, offers an observation that captures the complexity of the issue. According to him, the problem is not always a lack of resources. It is often social, geographical and cultural.
In districts like Nandurbar, he notes, families traditionally establish separate dwellings when children grow up. The physical distance may appear small on a map, but because settlements are scattered across undulating hills and ridges, travelling from one hamlet to another can take hours. Some padas have fewer than fifty residents. Some are located on hilltops. Others are separated by streams, valleys and forested terrain. “How many roads can one construct?” Dr Vyas asks, highlighting the difficult questions that policymakers face. His observation challenges a common assumption.
Urban India often measures development through infrastructure alone. Build a road, erect a hospital, install a mobile tower and the problem is solved. But tribal Maharashtra presents a more complicated reality. A road may reach a village. Yet dozens of smaller hamlets may still remain beyond easy access. A Primary Health Centre may exist. Yet the patient may need to walk for hours before reaching transport. An ambulance may be available. Yet the ambulance may not be able to reach the patient. This gap between infrastructure on paper and accessibility on the ground lies at the heart of the tribal health challenge.
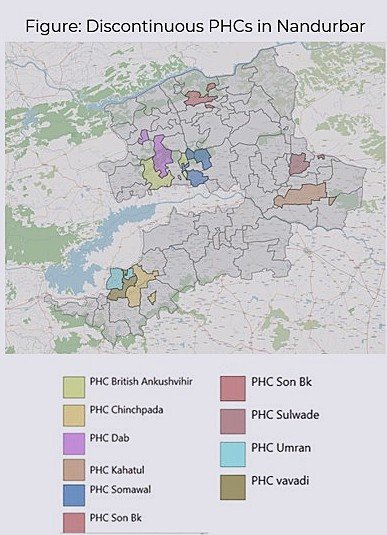
The Committee’s report highlights this through one striking example from Nandurbar district. Maps of Primary Health Centre jurisdictions reveal what health planners describe as “discontinuous catchment areas” — service areas fragmented by geography rather than connected through convenient transport routes. A health facility may officially serve a population spread across difficult terrain, making routine healthcare delivery far more challenging than conventional planning models assume. For health workers, reaching beneficiaries often becomes an expedition. For patients, seeking treatment becomes a journey and during medical emergencies, distance itself can become a health risk.
This is where the story of tribal health begins to move beyond hospitals and into the broader question of development. Because in many parts of tribal Maharashtra, the first battle is not against disease. It is against geography.
The challenge becomes even clearer when one looks at how healthcare actually reaches tribal communities. In urban India, healthcare is largely facility-based. Patients travel to hospitals. Doctors remain in clinics. Diagnostic services operate from fixed locations. The system assumes that people can reach healthcare. In tribal Maharashtra, the reality is often the opposite. Healthcare frequently has to travel to the people. Vaccination teams climb hills. ASHA workers walk long distances. Health staff cross streams and forest paths. Mobile outreach programmes become critical links between remote communities and the formal health system.

The Maharashtra State Tribal Health Committee Report documents several examples of healthcare personnel travelling through difficult terrain to conduct immunisation drives, maternal health monitoring and community outreach programmes. The photographs included in the report tell a story that statistics alone cannot. In one image, healthcare workers are seen conducting field activities under a tree in a remote tribal settlement. In another, teams travel across water bodies to reach isolated populations. These images reveal a reality often hidden behind administrative terminology such as “last-mile delivery”.
The last mile in tribal Maharashtra is rarely just a mile. Sometimes it is a mountain. Sometimes it is a forest. Sometimes it is a river and sometimes it is a journey that consumes an entire day. This reality helps explain why healthcare indicators cannot be viewed in isolation from infrastructure. The challenge is not always the absence of services. Often it is the difficulty of delivering them consistently.
Former Public Health Minister Dr. Deepak Sawant has spent years working on tribal health issues and his observations provide important context to the Committee’s findings. According to Dr. Sawant, many health interventions that appear straightforward in urban settings become considerably more complex in remote tribal regions. Take Home Ration programmes, for example, are designed to improve nutrition among mothers and children. Yet delivering these supplements to remote hamlets remains a logistical challenge.
During the monsoon, access routes are frequently disrupted. In some areas, supplies have to be transported in bulk because repeated journeys become difficult. The challenge then shifts from delivery to utilisation and quality preservation. Similarly, healthcare access cannot be measured only by the existence of facilities. A Primary Health Centre may function effectively. A doctor may be available. Medicines may be stocked. Yet if reaching that facility requires hours of travel, the practical accessibility of healthcare remains limited.
This is particularly important in maternal and child health. A pregnant woman requiring routine antenatal care can sometimes postpone a visit. A child requiring immunisation may be reached through outreach efforts. But emergencies do not wait for outreach programmes. Complications during pregnancy, severe fever, snake bites, accidents or acute illness demand immediate access and immediate access is precisely where geography exerts its greatest influence.
The report’s observations from tribal districts repeatedly highlight the tension between service availability and service accessibility. The two are not always the same. A health planner may count facilities. A tribal family experiences distance. This distinction is crucial for understanding why improvements in healthcare indicators sometimes occur more slowly than policymakers hope. Because the challenge is not simply building institutions. It is connecting people to those institutions.
The Committee’s work demonstrates that substantial progress has been made. Institutional deliveries have increased. Maternal mortality has declined. Child health indicators have improved. Public health outreach has expanded significantly over the past two decades. These achievements deserve recognition. Yet the report also suggests that future gains may increasingly depend on overcoming geographical barriers rather than merely expanding programmes.
The next phase of tribal health development may not be about creating entirely new schemes. It may be about ensuring that existing schemes can consistently reach every settlement, every family and every child. That is where the discussion begins to move beyond healthcare policy and into a larger conversation about roads, transport, communication and connectivity. Because sometimes the success of a health programme depends not on what happens inside a hospital. But on whether a patient can reach the hospital at all.
Some reports are remembered for their statistics. Others are remembered for the stories they tell. The Maharashtra State Tribal Health Committee Report contains photographs that say more than pages of data ever could. In one image, villagers are seen carrying a patient through a rocky forest path. In another, people wade through a river while transporting a person in a makeshift stretcher. There is no need for an elaborate explanation. The message is immediate.
Before treatment can begin, the patient must first survive the journey. For many urban readers, such images may appear extraordinary. For many tribal families, they are part of life. These photographs illustrate a truth that policymakers, administrators and public health experts have grappled with for decades: healthcare access is ultimately about mobility. A hospital bed has little value if a patient cannot reach it. An ambulance has limited utility if roads do not connect settlements. A doctor cannot treat a patient who remains beyond the reach of the healthcare system. This is why the Committee’s report repeatedly returns to the question of connectivity.
Not merely roads. Not merely transport. But the broader challenge of connecting isolated communities to essential services.
Former Public Health Minister Dr. Deepak Sawant recalls one such effort during his tenure. Recognising that conventional ambulance services could not reach many remote tribal settlements, his department introduced motorcycle ambulance services in certain areas. The idea was simple. If a four-wheeler could not reach the patient, perhaps a smaller and more agile vehicle could. The initiative reflected a reality often overlooked in policy design. Solutions for tribal regions cannot always be copies of solutions designed for cities. The terrain demands innovation. Yet Dr. Sawant also points to another reality. Many such initiatives struggle to survive because of funding constraints, administrative continuity and operational challenges.
Projects begin with enthusiasm. Maintaining them over the long term is often more difficult. His observation highlights a recurring theme running through the Committee’s report. The challenge is not merely creating programmes. It is sustaining them. The same applies to communication infrastructure.
In remote regions, poor mobile connectivity can delay emergency response. A family facing a medical emergency may not always be able to call for help immediately. Health workers may find it difficult to coordinate transport. Referral systems that function smoothly in urban areas become more complicated when communication itself becomes uncertain. The consequences are most visible during emergencies. A complicated pregnancy. A child with severe illness. A snake bite. An accident. A medical condition that requires immediate referral. In such moments, every minute matters. And every kilometre matters.
The Committee’s report does not suggest that these challenges are insurmountable. On the contrary, it documents substantial progress. Health indicators have improved. Institutional deliveries have increased. Maternal mortality has declined. Child survival has improved significantly over the past two decades. These are important achievements. But the report also reminds us that averages can sometimes hide realities.
State-level progress does not eliminate local hardship. Development can advance while pockets of exclusion remain and tribal Maharashtra continues to contain some of those pockets. Perhaps that is why the observations of Dr. Pradeep Kumar Vyas carry particular significance. His argument is not that the government has failed to build infrastructure. Rather, it is that geography itself imposes limits that conventional planning struggles to overcome. When populations are scattered across hills, forests and remote hamlets, service delivery becomes fundamentally different. The challenge is not only financial. It is structural. It is geographical and in many ways, it is human.
The Tribal Maharashtra series began with a simple question: Who are the one crore tribal citizens of Maharashtra? Over the past four parts of this journey, the answer has gradually unfolded. They are citizens who have witnessed improvements in healthcare, nutrition and public services. They are communities whose children are surviving in greater numbers than before. They are families who have benefited from decades of public investment and social programmes. But they are also citizens for whom development often travels a longer road.
A mother waiting for antenatal care. An ASHA worker climbing a hill to reach a hamlet. A vaccination team crossing difficult terrain. A patient being carried towards help. These are not merely images from a report. They are reminders that development is ultimately measured not by policies announced or budgets allocated, but by whether public services reach those who need them most.
In cities, distance is usually measured in kilometres. In tribal Maharashtra, distance is often measured in opportunity. The distance between a hamlet and a hospital. The distance between a child and healthcare. The distance between policy and implementation. The distance between promise and delivery. Bridging that distance may be one of the most important development challenges Maharashtra faces in the years ahead. Because for many tribal families, the first battle is not against disease. Sometimes, it is against distance itself.

{kind=link}